Brief Case Description
The patient is a 33 year-old male with a past medical history of rheumatic fever who presented with dyspnea on exertion. He also has a history of paroxysmal atrial fibrillation.
Transthoracic echocardiography (parasternal long axis and four-chamber views) showed type IIIa mitral valve dysfunction (restricted leaflet motion in diastole and systole) involving the posterior leaflet. The posterior leaflet was significantly thickened and retracted. The anterior leaflet mobility was preserved. On Doppler echocardiography, there was severe mitral regurgitation with a posteriorly directed jet. Quantitative measurements showed an effective regurgitant orifice area (ROA) of 72 mm2 and a regurgitant volume of 51 mL. Pisa radius was 1.1 cm. There was also moderate mitral stenosis with a valve area of 1.4 cm2 by Doppler echocardiography.
There was also Type I tricuspid valve dysfunction with mild regurgitation. Left ventricular end diastolic diameter was increased to 6.3 cm. Left ventricular ejection fraction was 65%. Right ventricular function and size were normal.
The patient was referred for reconstructive mitral and tricuspid valve surgery, and biatrial maze procedure.
Preoperative cardiac catheterization showed normal coronaries. The mean transmitral gradient was 8 mmHg. The mitral valve area was calculated at 1.4 cm2. Pulmonary artery pressure was 50/26 mmHg.
Operative Procedure
Intraoperative Transesophageal Echocardiography
Intraoperative transesophageal echocardiography confirmed the diagnosis of type IIIa mitral valve dysfunction. Mid esophageal long axis view showed type IIIa dysfunction with the thickening and retraction of the posterior leaflet. Similar findings were observed in mid esophageal mitral commissural view. Mid esophageal long axis and four-chamber views with color Doppler interrogation of the mitral valve showed a posteriorly directed jet and mitral regurgitation was graded severe. The mobility of the anterior leaflet was preserved, which is an important consideration for reconstructive valve surgery. The height of the anterior leaflet at the level of A2 segment was 2.8 cm. Mitral annular diameter was measured at 4.2 cm.
Mitral Valve Analysis
Following the left atriotomy, annular sutures were placed to improve the mitral valve exposure. Intraoperative valve analysis confirmed the findings of echocardiography by demonstrating type IIIa dysfunction with typical rheuamtic valve lesions. They were multiple, complex and could be described as follows (Left video):
Following this complete echocardiographic and operative valve analysis, we can summarize the pathophysiological triad as follows:
Etiology: Rheumatic valve disease
Lesions: Anterolateral commissural fusion, posterior leaflet thickening and retraction, minimal subvalvular lesions (chordae thickening), associated annular dilatation
Dysfunction: Type IIIa- posterior leaflet
Reconstructive Procedure
Valve reconstruction was considered feasible in this case as the anterior leaflet had a preserved surface area and mobility and the subvalvular lesions were minimal.
First, an anterolateral commissurotomy was performed. Traction on the chordae of the anterior and posterior leaflets allowed us to identify precisely the fused commissure. Using a knife, the incision started a few millimeters from the annulus and was directed towards the mitral valve orifice. The commissural chordae was divided, leaving a marginal chordae on each side of the commissural opening. As shown below, we created a large orifice which admitted the extremity of the surgical forceps. We can also observe in this video that subvalvular lesions were minimal.
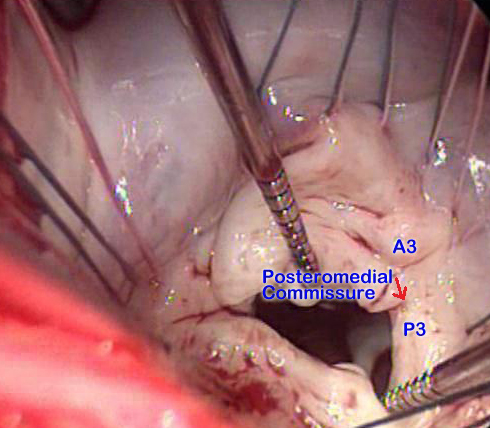
We also inspected the posteromedial commissure which displayed minimal fusion and therefore was left intact.
The posterior leaflet was transversally incised from mid-P1 to mid-P3 segment a few millimeters from the annulus. The adequate exposure of the ventricular aspect of the leaflet enabled us to resect all secondary chordae attached to the posterior leaflet to increase its mobility (Left video). An oval-shaped glutaraldehyde preserved autologous pericardial patch was tailored and used for extension of the posterior leaflet. The maximum height of the patch was 14 mm and its length was equal to the length of the detached posterior leaflet. The 14 mm height was calculated in order to obtain a maximum posterior leaflet height of about 2 cm. The pericardial patch was inserted using a 4/0 monofilament suture in a running fashion (Right video).
Finally, a prosthetic ring annuloplasty was performed. Ring selection is based on the measurement of the intercommissural distance and the surface area of the anterior leaflet. A 32 mm sizer was chosen to measure the intercommissural distance and was the right sizer. The same 32 mm sizer was then selected and covered the entire surface area of the anterior leaflet (Left video). The selected ring, however, should take into consideration the surface area of the reconstructed posterior leaflet. The use of patch extension enabled us to implant a 34 mm Carpentier Edwards Physio ring (one size greater than the sizer covering the anterior leaflet) (Right video).
Furthermore, the patient underwent a tricuspid remodeling annuloplasty with a 32 mm Carpentier Edwards Physio tricuspid ring for type I dysfunction due to annular dilatation. A concomitant biatrial cryomaze procedure was also performed.
Postbypass Transesophageal Echocardiography
Mid esophageal long axis and four-chamber views showed the prosthetic ring in place with an increased surface of coaptation. Mid esophageal long axis and four-chamber views with color Doppler interrogation of the mitral valve showed a competent valve with no residual regurgitation. The peak transmitral gradient was 6 mmHg. Three-dimensional rendering of the mitral valve also showed an excellent result. The pericardial patch could be visualized on ventricular view.